
Dorsal Hump Rhinoplasty
Dorsal hump rhinoplasty is frequently requested, but selecting and executing the optimal treatment plan for each patient can be a complex endeavor. There are a number of surgical techniques that can be employed for dorsal hump rhinoplasty. Dr. David Cangello, a highly sought after rhinoplasty surgeon in New York City, is an expert in dorsal hump rhinoplasty and one of the first plastic surgeons in the United States to offer preservation rhinoplasty.
Defining Aesthetic Goals of Dorsal Hump Rhinoplasty
While a surgeon must take into account the unique anatomy and cosmetic goals of each patient, there are several aesthetic principles that apply in most dorsal hump rhinoplasty cases. The goal in all cases is a straight profile with a natural-looking nasal tip. Patients seeking dorsal hump rhinoplasty often present with a dorsal hump deformity, the placement and level of which will factor into a surgical plan.
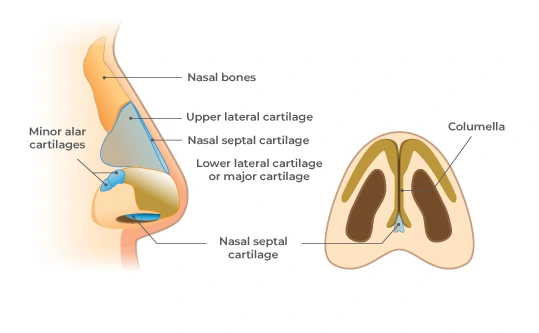
The Nasal Keystone Area
Any successful dorsal hump surgery must meticulously approach and maintain the keystone area of the nose. The keystone area, which is located where the upper lateral cartilage and nasal bones meet the septum, is critical in supporting the structural stability of the dorsum. This area consists of nasal bone, cartilaginous septum, bony septum, and upper lateral cartilages.
Tip Refinement in Dorsal Hump Rhinoplasty
A supra-tip break, in which a slight upward angulation at the point where the bridge connects with the tip, is appropriate for most female dorsal hump rhinoplasty patients. It should, however, be avoided in most male patients as it can appear overly feminine. A conservative approach should be taken with the supra-tip break to avoid a “scooped out” or “ski jump” appearance. A tip projection of approximately a millimeter beyond the dorsum creates a pleasing aesthetic in many female patients.
Preservation Methods for Dorsal Hump Rhinoplasty
Dr. Cangello finds that approximately 50% of his dorsal hump patients are good candidates for preservation rhinoplasty. There are several kinds of preservation rhinoplasty that can be used for dorsal hump procedures.
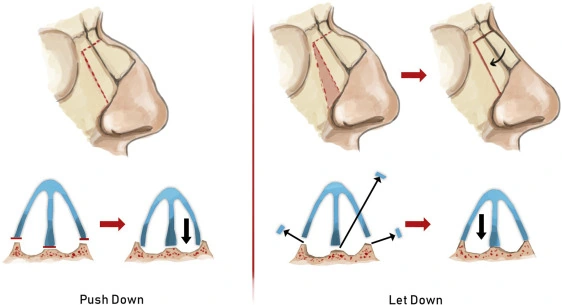
Cottle Push Down Technique
This technique was originally developed by Dr. Maurice H. Cottle in response to complications he saw as a result of traditional rhinoplasty methods that involved removal of the roof of the nasal dorsum.1 The Cottle technique preserves the dorsum and makes use of the flexible chondro-osseous joint that sits between the cartilaginous vault and the nasal bones. In this manner, small to medium nasal humps and bridge irregularities can be corrected while minimizing trauma and functional complications as well as aesthetic ones.
Let Down Rhinoplasty with Modified Cottle Technique
Since it was first introduced in 1954, several modified versions of Cottle’s technique have been introduced. Dr. Cangello often performs let down rhinoplasty with a modified Cottle technique. This approach improves upon the original Cottle technique by avoiding the nasal obstruction that can sometimes occur with a push down method. 2
In this approach, Dr. Cangello typically begins with a septoplasty, including septal disarticulation from the ethmoid bone and ethmoid wedge resection. The ethmoid wedge resection is made just under the nasal bridge so that once osteotomies are made, the bridge can be “let down.” Osteotomies are then performed to mobilize the dorsum. While a pushdown technique uses a transverse osteotomy and a single lateral osteotomy on each side, the let down technique uses two lateral osteotomies on each side, which allows for resection of a wedge shaped piece of bone. In turn, this allows for better adaptation of the nasal pyramid, once it is let down. A radix osteotomy then follows and this creates a hinge which allows the nasal keystone/dorsum to be moved downward or “let down” en bloc. The dorsal height can then be adjusted to the optimal position.
Ishida Push Down/Spare Roof Technique(s)
For larger noses and those with deviated humps or irregular nasal bones which do not create beautiful dorsal aesthetic lines, the Ishida push down or Spare Roof technique may be used. These approaches focus on the cartilaginous mid-third of the nose and may or may not (respectively) preserve the bony cap of the keystone area. Case studies show that nasal humps are successfully corrected with these techniques for more than 95% of patients.3
The Ishida technique uses two osteotomies on the keystone nasal bones, beginning at the widest point and extending to the midline. This effectively allows separation of the bony cap from the nasal bones and preserves it. With the Spare Roof technique, the bony cap is removed. In either case, the cartilaginous portion of the hump can then be lowered while it is left completely intact. The length of dissection and release of the upper lateral cartilages from the nasal bones between the nasal aperture and the lateral keystone area will determine how far the dorsum is lowered.
Traditional Dorsal Hump Rhinoplasty
Traditional hump reduction techniques involve separating the upper lateral cartilages from the nasal septum. This is very different from preservation techniques where the cartilaginous portion of the dorsum remains completely intact (hence the ULCs are not separated from the septum). With traditional (which is also referred to as “structural”) dorsal hump rhinoplasty techniques, the upper lateral cartilages and the dorsal septum are then trimmed in order to excise the portions that create the hump. Spreader grafts are sometimes necessary and the nasal dorsum must be reconstructed, with reattachment of the upper lateral cartilages to the nasal septum, once they have been resected, in order to maintain the nasal structure. Spreader grafts are never needed when preservation techniques are used and the dorsum need not be reconstructed since it is left intact. These are advantages of preservation rhinoplasty.
Determining an Optimal Treatment Plan for Dorsal Hump Rhinoplasty
In general, patients who are seeking a revision rhinoplasty will be best suited to a more traditional approach as they will not be candidates for any preservation method. Candidacy for various preservation techniques will depend on the width of dorsum and the composition and height of the hump deformity. Dr. Cangello takes several factors into account when determining what approach is best for an individual patient’s needs and goals. He also uses advanced tools, including Piezo ultrasonic rhinoplasty that allows for precise cutting of bone (osteotomies) and shaping of bone while preserving soft tissue. Piezo can not and does not harm soft tissue surrounding the bone, while chisels can cause damage as they are guided through their paths to create osteotomies.
References
1 Mayo Clinic. Rhinoplasty. Available here: https://www.mayoclinic.org/tests-procedures/rhinoplasty/about/pac-20384532. Accessed 11/6/2019.
2 Montes-Bracchini JJ. Nasal Profile Hump Reduction Using the Let-Down Technique. Facial Plast Surg. 2019 Oct;35(5):486-491. doi: 10.1055/s-0039-1695751. Epub 2019 Oct 22. PMID: 31639873.
3 Luiz Carlos Ishida, MD, PhD, Jorge Ishida, MD, PhD, Luis Henrique Ishida, MD, PhD, Adriane Tartare, MD, Rafaela Katerine Fernandes, MD, Rolf Gemperli, MD, PhD, Nasal Hump Treatment With Cartilaginous Push-Down and Preservation of the Bony Cap, Aesthetic Surgery Journal, Volume 40, Issue 11, November 2020, Pages 1168–1178, https://doi.org/10.1093/asj/sjaa061
1 Mayo Clinic. Rhinoplasty. Available here: https://www.mayoclinic.org/tests-procedures/rhinoplasty/about/pac-20384532. Accessed 11/6/2019.
2 Montes-Bracchini JJ. Nasal Profile Hump Reduction Using the Let-Down Technique. Facial Plast Surg. 2019 Oct;35(5):486-491. doi: 10.1055/s-0039-1695751. Epub 2019 Oct 22. PMID: 31639873.
3 Luiz Carlos Ishida, MD, PhD, Jorge Ishida, MD, PhD, Luis Henrique Ishida, MD, PhD, Adriane Tartare, MD, Rafaela Katerine Fernandes, MD, Rolf Gemperli, MD, PhD, Nasal Hump Treatment With Cartilaginous Push-Down and Preservation of the Bony Cap, Aesthetic Surgery Journal, Volume 40, Issue 11, November 2020, Pages 1168–1178, https://doi.org/10.1093/asj/sjaa061